The New Healthcare Workforce: Will Form Follow Function?
Posted on | December 4, 2013 | Comments Off on The New Healthcare Workforce: Will Form Follow Function?
Mike Magee
In the November 21, 2013 issue of the New England Journal of Medicine, the lead article asks, “Are We in a Medical Education Bubble?”(1) In the article, the authors explain that “ Bubble markets are created when an asset trades for increasingly higher prices as it is bought by people who are hopeful about its future value and then sold to others with even more optimistic views of that value.”
They then go on to describe the specific case of medical students who assume debt to attend medical school and residency programs (where they are compensated at under-market rates) in anticipation of future value.
To put a number on their predicament, the authors use the ratio of the “average debt of a graduating student/resident to the average (1st year) income in the profession on entry into the workforce”. As might be expected, Family Medicine fared the worst (graduating on average with a debt burden approaching 90% of their 1st year salary), while orthopedics, cardiology and radiology fared the best (graduating with a debt burden that was less than 1/3 their 1st year salary).(1)
No surprise. But then came the graph below which painted healthcare human resources with a broader stroke, and made Family Medicine look pretty good.
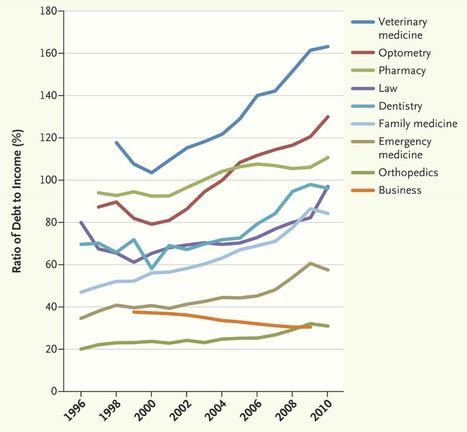
Here we see Veterinarians with crushing debt (160%), and Optometry (130%), Pharmacy (110%), and Dentistry (approaching 100%) not far behind.
The authors go on to make a couple of not too subtle (and not entirely defensible) points.
1) They say, “The general lesson is that if we want to keep health care costs down and still have access to well-qualified physicians, we also need to keep the cost of creating those physicians down by changing the way physicians are trained.”
2) And also say, “Although it seems unlikely that we’re in a bubble market for medical education, we may already be in one for veterinary medicine.”
Reality Check: The market is somewhat rigged as many medical students come from affluent families that subsidize their investment to a considerable extent. Futhermore, those entering Medicine and other health related fields seek a variety of intangibles beyond financial reward including standing in their communities, stable lifetime employment, and challenging work that directly and positively impacts other human beings.
That said, physician organizations say we need more doctors. The Association of American Medical Colleges says we’ll be short 62,900 doctors by 2015.(2) Inspite of the crushing debt imposed on graduating medical students and the delayed earning power resulting from an additional 3 to 5 years of residency training after medical school graduation, tons of kids still want to go to medical school. This helps explain, in part, why 16 new medical schools have opened in the past decade with another 12 in development.(2) To do what? To largely train kids how to practice medicine the way it has always been practiced – rather then as it soon will be practiced.
Aging, the Internet, health consumerism and universal health insurance coverage all point to a future home-centered health care system focused on individual and family responsibility and individualized preventive strategic health planning.(3)
Of the many challenges this end point entails, none is more serious than human resources – creating an affordable and efficient workforce that is up to the task. This likely will require new job descriptions for every caring professional including the physician, massive retraining of existing workers, and critical re-thinking of workforce plans for new entrants into the various health care fields.
Health policy expert John K. Iglehart said as much in a 2011 article in the New England Journal of Medicine noting that health care human resource issues are rapidly coming to a head.(2) In that article Bill Frist is quoted as saying, “To meet the explosive demand of primary health services will require a truly disruptive reform of how primary care is delivered. Delivering primary care will not remain the sole purview of doctors. There are not enough of them, and they are too expensive.”(2)
And seemingly in response, Dr. Darrell Kirch, CEO of the Association of American Medical Colleges, is quoted “…This creates an imperative for academic medical centers to respond with new approaches to training, as well as research regarding which educational and care models work best.”(2)
Iglehart is right – healthcare human resources are very much the issue. But health care leaders (even in the midst of the messy role-out of Obamacare which is certain to be transformative) continue to signal an inability to see the new health care forest through the historical health provider trees.
To get it right, they need to answer these 5 questions.
1. What kind of health delivery system do we want to build?
2. How will we manage our chronic disease burden while simultaneously emphasizing prevention and strategic health planning beginning at conception?
3. How do we position universally insured Americans to perform optimally as both providers and consumers of care?
4. What is the “job description” of the individual, the family, and the community – and how are these integrated into the new health care team?
5. How do we advantage mobility and technologic reach to reinforce knowledge transfer, continuity planning, coaching, data transfer and analysis, and research to maximize quality and efficiency; and what percentage of the new healthcare workforce should be mobile and exhibit home penetrance?
Do we need doctors? Of course – just as we need veterinarians, dentists, optometrists and pharmacists. But to determine how many of these, and what kind of “others” requires an extraordinarily broad and wise vision – especially as Obamacare sets the health care pieces in motion.
When it comes to healthcare workforce planning, experts would do well to internalize the golden rule of successful architects and designers: “Form Follows Function.”
For Health Commentary, I’m Mike Magee
References:
1.Are We in a Medical Education Bubble Market . Asch DA et al. N Engl J Med 2013; 369:1973-1975, November 21, 2013DOI: 10.1056/NEJMp131077. http://www.nejm.org/doi/full/10.1056/NEJMp1310778
2. Iglehart JK. The Uncertain Future of Medicare and Graduate Medical Education. http://www.nejm.org/doi/full/10.1056/NEJMhpr1107519
3.Magee M. “Connecting Healthy Homes To a Preventative Health Care System: Leveraging Technology For All Its’ Worth”,
Harvard Health Policy Review, Nov. 2007. http://hhpronline.org/publication/previous-issues/fall-2007-part-1/
Tags: bill frist > darrell kirch > health industry > healthcare workforce > human resources > John Ingelhardt > medical education bubble > NEJM > new england journal of medicine > Obamacare
Comments
"Code Blue INDEX online"

![]()
![]()
Prospective Health Blog
BIOGRAPHY
Homegrown Friends
BIOGRAPHY
NIH Precision Medicine
BIOGRAPHY
Health in 30
BIOGRAPHY
Larry's Letters
BIOGRAPHY
Precision Medicine, Euthanasia, Abortion, Communism, Trillions of Dollars, Losing Freedom, and Town Hall Mobs BIOGRAPHY
Yearning for Universal Coverage Is Not Universal
BIOGRAPHY

