The Winning Argument For Universal Health Care Is Economic Not Ethical.
Posted on | August 3, 2017 | 2 Comments
 (Check out your state HERE)
(Check out your state HERE)
Mike Magee
The optimistic top line headlines today dominated health news even while Congress struggles on the very basics of health delivery. “U.S. scientists fix disease genes in human embyos for the first time” blares USA Today. But turn to the Opinion page and you’ll find “Trump admits that sabotage is real Republican health care plan.”
What these competing headlines make clear once again is that scientific progress is not synonymous with human progress. Our faith in free enterprise and capitalism to “win the war” on disease (and supposedly leave “health” in its wake) dates back to the immediate post – WWII era. Over the years we’ve doubled down on this historically poor decision again and again, breeding profiteers, colluders, and promoters – but not much health for America.
The historic intermingling of health and business has yielded a long list of side-effects including: academic medicine’s rush for NIH grants, sellable patents, DTC advertising and AMA profiteering database sales, industry’s relentless assault on checks and balances and their expanding government relations, and government’s open door policy toward scientists with well known conflicts of interest. All spell success for the ever expanding Medical-Industrial Complex, but treat patients as pawns.
The cast of characters and drama that is unfolding resembles the Soviet Union’s demise on December 26, 1991. For a solid decade preceding this event, the power elite of that federation vigorously defended their status quo and the reckless build up of their military spending which eventually sent them over the financial cliff. Our misdirection of American healthcare is heading rapidly toward a similar endpoint.
The winning argument for a restructuring of our healthcare system and the movement toward single payers is economic not ethical. Universal coverage is necessary not because it’s a human right (which it is), but because risk must be shared to make insurance work, and uncovered citizens ultimately cost society more – much more! A healthy population is more productive, more likely to be educated, more mobile and willing to take risk, more likely to get married and have children, less likely to be involved in crime, violence, or injury. And all of this saves money.
When Warren Buffett said that “Medical costs are the tapeworm of American economic competitiveness”, he knew what he was talking about. But to responsibly transition ourselves out of this mess requires two things: 1) a vision/strategic plan, 2) the capacity to retrain and redirect health care workers from reactive health delivery to proactive and preventive social services.
On the vision front, studies clearly indicate that consolidating administrative back-office management of insurance sales, benefit management, and claims payments could immediately shave 15% off our national health care bill. But getting there is not as easy as uttering the magic phrase, “Medicare-for-all”. Let’s remind ourselves that while Medicare is quite efficient compared to private insurers, it is not a single-payer system. One third of Medicare enrollees voluntarily participate in Medicare Advantage plans run by private companies who receive special incentives and subsidies out of our tax dollars. The good news is that the government attaches strings to the deal like enforced caps on out-of-pocket expenses. Also one fourth of enrollees have supplemental “Medigap” policies.
Seniors strongly support Medicare as it exists, as do many employees who receive insurance as a work benefit. So when we begin to think about moving to a single payer, we need to think about an incremental option that allows those who wish to switch versus brute force. A huge change like this will take time, and flexibility is our friend not our enemy. For example, Canada leaves the planning, prioritization and delivery of care in their “single-payer” system in the hands of the separate provincial governments. This is not dissiliar to the way we expanded Medicaid, providing baseline standards and financial subsidies from the federal government but giving each governor the authority to balance and integrate local health delivery with a range of other social services. Having local control of both buckets may be essential in transitioning workers in the near future.
Workforce transition is at least as great a challenge as shared responsibility. For every one physician in America, there are 16 additional health care workers. Approximately half of them are non-clinicians uninvolved in hands-on care. And not all the clinicians actually care for patients either. Name brand doctors in big academic centers today, touting “personalized medicine” this and “personalized health” that often more closely resemble dot-com entrepreneurs than the hands-on caregivers making rounds and teaching house staff of years gone by.
Health care now includes 11% of all workers compared to 8% in 2000. Since the country’s near financial collapse in 2007, 35% of the job growth has been in health care, fueled by aging demographics and the expansion of Medicaid under the ACA. More than 1/2 of the nearly $4 trillion spent on health care in the U.S. goes to wages. You can find a list of some the jobs, along with average salary and educational requirements HERE. The American Academy of Professional Coders is now nearly 200,000 strong with average salary approaching $50,000 a year. Near 20% growth in healthcare jobs is projected by the government in the coming decade, adding an additional 2.3 million positions is we maintain the status quo.
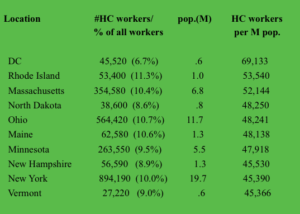
Shifting toward universality, planning, prevention, and efficient management will be profoundly disruptive to many workers. The impact would vary from state to state depending on their historic over-weighting of the health care sector. For example, listed above are the top ten states (including D.C.) ranked by the highest number of health sector workers (excluding those self-employed) per million citizens. The D.C. outlier reflects the Medical-Industrial Complex’s commitment to self-interest lobbying. States like Massachusetts, Rhode Island and New York have large academic enterprises with active industry partners. States like North Dakota, Maine, New Hampshire and Vermont have small widespread rural populations many of whom are economically vulnerable.
The point is, adjustments of work force in response to substantitive health care reform would need to be addressed on the local level and would be a significant challenge to state governors.
A starting point would be to deconstruct enterprises which primarily service direct care needs from those engaged in speculative scientific discovery for profit. These are radically different entities. Step two would be to integrate direct patient care with the continuum of social services. Plan for health, not disease. Finally, be bold. If we want to avoid Russia’s fate, change must be our friend.
Tags: health and economics > health care crisis > health care workers > health care workforce > healthcare reform > medical-industrial complex > single payer > warren buffett
Comments
2 Responses to “The Winning Argument For Universal Health Care Is Economic Not Ethical.”
"Code Blue INDEX online"

![]()
![]()
Prospective Health Blog
BIOGRAPHY
Homegrown Friends
BIOGRAPHY
NIH Precision Medicine
BIOGRAPHY
Health in 30
BIOGRAPHY
Larry's Letters
BIOGRAPHY
Precision Medicine, Euthanasia, Abortion, Communism, Trillions of Dollars, Losing Freedom, and Town Hall Mobs BIOGRAPHY
Yearning for Universal Coverage Is Not Universal
BIOGRAPHY


August 4th, 2017 @ 8:58 am
Great article.
August 4th, 2017 @ 9:02 am
Thanks, Karl. Means a great deal coming from you! Mike