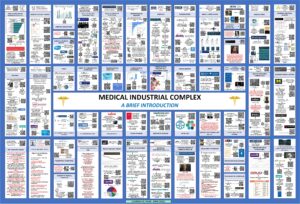
The MIC in Schematic Design with QR2 Interactive Reference Codes.
Posted on | September 2, 2021 | Comments Off on The MIC in Schematic Design with QR2 Interactive Reference Codes.
Laurence M. Raine DrPH is a Senior Science Analyst with the Department of Homeland Security with extensive research and governmental experiences in the life sciences. He holds a Doctorate in Public Health, a Masters in Botany, and a Certificate in Scientific and Technical Illustration. What Larry enjoys is creating detailed integrated system schematics to describe complex subjects like the Medical Industrial Complex. Here is the MIC through Dr. Raine’s eyes complete with interactive QR2 reference codes. (lmraine@gmail.com)
Source: Academia. Access to Download.
“Metaverse” – What’s In The Word?
Posted on | September 2, 2021 | 4 Comments
Mike Magee
Keying in on words is a habit that dates back to Medical School. From 1969 to 1973, in Syracuse, NY, (experts estimate) I absorbed 15,000 new vocabulary words as part of my training.
dystopian
[disˈtōpēən]
ADJECTIVE
- relating to or denoting an imagined state or society where there is great suffering or injustice.
NOUN
- a person who imagines or foresees a state or society where there is great suffering or injustice.
There are certain words that keep popping up in 2021 whose meanings are uncertain and which deserve both recognition and definition. And so, the offering above – the word “dystopian.” Dystopian as in the sentence “The term was coined by writer Neal Stephenson in the 1992 dystopian novel Snow Crash. “
One word leads to another. For example, the above mentioned, dystopian term, referenced by science fiction writer Stephenson three decades ago, was “Metaverse”. He attached this invented word (the prefix “meta” meaning beyond and “universe”) to a vision of how “a virtual reality-based internet might evolve in the near future.”
“Metaverse” is all the rage today, referenced by the leaders of Facebook, Microsoft, and Apple, but also by many other inhabitors of virtual worlds and augmented reality. The land of imaginary 3D spaces has grown at breakneck speed, and that was before the self-imposed isolation of a worldwide pandemic.
But most agree that the metaverse remains a future-facing concept that has not yet approached its full potential. As noted, it was born out of science fiction in 1992, then adopted by gamers and academics, simultaneous focusing on studying, applying and profiting from the creation of alternate realities. But it is gaining ground fast, and igniting a cultural tug of war.
Today multinational corporations are all in. Jason Warnke of giant consulting firm Accenture sees it as a power enhancer and multiplier. He says “…we believe we now have the opportunity to bring our people together in ways never before possible in the physical world.”
Not so fast, says Esther O’Callahan, the Gen-X founder of the online recruitment firm Hundo. She says the term is“… owned by young people who care more about community than profit and use it for the good of the real and virtual world. And if that sounds ludicrously naive and optimistic about it – I am and I’m not sorry!”
Karinna Nobbs, CEO of The Dematerialized, envisions the coming metaverse as a societal builder referring to it as “the next significant third space.” In doing so, she is appropriating a term made famous by sociologist Ray Oldenburg in his 1989 book, “The Great Good Place”. In it, the author advocates for investment in public spaces, outside of home and work that encourage congregation, civic engagement and relationship building. Karinna sees her virtual company as a “third space” to converge and nurture the emerging digital fashion ecosystem.”
Not surprisingly, health entrepreneurs are all over the metaverse as well. Or at least they think they are. Many of the new ventures are led by current or former health executives, attracted by investor demand, selling marginal moves in telemedicine, robotics, behavioral health, consumer wearables and the like.
Deloitte & Touche LLP report that digital health investment has quadrupled in the past four years, including $21.6 billion in 2020. They see health tech invasion of the metaverse as “a prescription for disruption by a growing base of health technology investors armed with funding from special-purpose acquisition companies (SPACs).” Investors are literally betting on an idea since SPACS go public without any existing business operations. They play to profit, not to disrupt.
Journalist turned tech analyst, AMP Creative’s Elena Piech sees the metaverse as “enabling us to be surrounded by information…this is the next iteration of life.” Could that work for health care, and if so, what might be the deliverables. Here are three:
Heal – When humans fall ill, they entrust doctors and nurses to respond in real time with knowledge, touch, and accessible resources. Could a health metaverse allow for a more ethical, equitable, efficient, inclusive and safer system of interventional care?
Health – Prevention and wellness benefit from patient-health professional relationships marked by compassion, understanding, and partnership. Could the metaverse reinforce trust and confidence, reliable information exchange, personalized health planning, and management of fear and worry?
Whole – Health is a function of a wide range of social determinants like housing, nutrition, clean air and water, education, and economic security. These resources are the products of good governance and healthy communities built around individuals, families, and societies. Could the metaverse, as a virtual “3rd space” contribute to community harmony, stability, security and happiness in a manner that kept us whole?
When it comes to a healthy metaverse, what then is the takeaway? Our health is not a game. It is our life. And as Esther O’Callahan said, “…if that sounds ludicrously naive and optimistic about it – I am and I’m not sorry!”
Tags: Deloitte & Touche > elena piech > esther o'callahan > gamers > health metaverse > jason warnke > karinna nobbs > metaverse > neal stephenson > ray oldenburg > snow crash > SPACS > tech health IT
What Comes After Delta?
Posted on | August 25, 2021 | 2 Comments
Mike Magee
“Many still see Alpha and Delta as being as bad as things are ever going to get. It would be wise to consider them as steps on a possible trajectory that may challenge our public health response further.”
Aris Katzourakis, Evolutionary Biologist, University of Oxford.
In my Jesuit high school, we were offered only one science course – chemistry. I took it in my Senior year and did pretty well. In contrast, I took four years of Latin, and three years of Greek, as part of the school’s Greek Honors tract.
Little did I know that Covid would create a pathologic convergence of sorts six decades later. Let’s review the Covid mutants:
Alpha – A variant first detected in Kent, UK with 50% more transmissibility than the original and has spread widely.
Beta – Originating in South Africa and the first to show a mutation that partially provided evasion of the human immune system, but may have also made it less infectious.
Gamma – First detected in Brazil with rapid spread throughout South America.
Delta – First seen in India with 50% more transmissibility than the Alpha variant, and now the dominant variant in America and around the world.
Our ability to track and identify mutating viruses in real time is now extraordinary. Over 2 million Covid genomes have been cataloged and published. But describing the “anatomy” of the virus is miles away from understanding the functional significance of their codes, or the various biochemical instructions they may instruct.
These deeper questions are in the realm of evolutionary biologists who are currently experiencing sleepless nights. Their recurrent nightmare? “What comes after Delta?”
What they know already is that Delta’s genetic mutation, P681R, affected a spot on the virus spike that cuts through protein chains and sped up human cell entry 1000 times. The speed lit a fuse under colony growth, which in turn allowed the virus’s spread to other unsuspecting human contacts before any immune response generated symptoms appeared. Of course the state of being asymptomatic didn’t last for long. Speedy virus multiplication rates accelerated the microbes movement from upper airways to lower airways leading to hospitalization rates that are twice as common as they were in the original Covid.
What’s next in the Greek alphabet? First a few basics.
1. A virus’s survival, and threat to us, relies on three factors:
a)Infectiousness, b) Virulence, c) Immune Evasion.
But these factors can as easily play against each other as for each other. Natural or vaccine induced immunity slows down infectiousness and potential virulence. But (by narrowing a virus’s options for survival) it also creates a Darwinian reward for any mutant that figures out the Rubik’s Cube solution to becoming “invisible” to the human immune system. According to Rockefeller University virologists, such a change requires the coalescence of 20 independent random changes in the genome. Bottom line: Random escape is a tall order. But under the current system, with Delta transmissibility likely to eventually burn through most of its potential future victims, such a change would be richly rewarded.
2. Viruses depend on us. But we no longer look or act as we did in 2019. Two billion citizens worldwide have had at least one dose of the vaccine, and hundreds of millions of others have survived the infection. The virus each day is increasingly pressured to find its next human victim. One way out is to figure a way past our immune defenses provided by prior infection or vaccination.
So this is a cyclical game, likely to go on for some time. If we global citizens play our vaccination cards right, the virus has fewer turns in the game, and is less likely to draw the cards it needs to evade our human defenses.
So here are five take-away facts:
- The longer we allow Covid to stick around, the worse this could get.
- The majority of the messy replication mistakes are inconsequential, but there are occasional windfalls that rise to Greek alphabet mythical status.
- Delta’s critical weakness – it leaves behind high antibody titers that limit its future.
- Give the virus more time, or access to compromised hosts, and anything can happen. Viruses are constantly rolling the evolutionary dice.
- Mutations hurt us by increasing transmissibility/virulence or immune evasion. The good news is there is some evidence that an immune escaping Covid might not be efficiently transmissible any more.
A guy like Ron DeSantis is not only ignorant of evolutionary biology, he’s playing with fire – and with our human lives. This cannot go unchallenged. Whatever it takes, we need to force this virus into a corner. Otherwise, we run the risk of becoming a Greek tragedy ourselves.
A Long Awaited “Moment of Truth” For FDR and President Biden.
Posted on | August 22, 2021 | 1 Comment
Mike Magee
A word is dead
When it is said,
Some say.
I say it just
Begins to live
That day.
Arguably, no President better understood the power of the word then FDR. When he structured up “a series of programs, public work projects, financial reforms and regulations…to provide support for farmers, the unemployed, youth and the elderly”, he memorably packaged the plan under the label, “The New Deal.”
Seizing alliteration in 1933, he further defined his new policies as the “3 R’s – Relief, Recovery, Reform”, promising “…action, and action now.”
When corporate America began to coalesce against him in 1936, he once again chose his words carefully in the public defense. Seizing the largest venue he could find at the time – Madison Square Garden – he stood tall and erect, supported by heavy leg braces, and declared defiantly, “They are unanimous in their hate for me – and I welcome their hatred.”
As he aged and his general health declined, his will to serve and honor his commitment to serve the American people only grew. With a heavy dose of humility and learned wisdom, he rose again on January 11, 1944, fifteen months before his death, and delivered the State of the Union Address as a Fireside Chat from the Oval Office in the White House. His words once again were clear and ever lasting. He stated that the original Bill of Rights was “inadequate to assure us equality in the pursuit of happiness.”
Powerful words, in their messaging and meaning, survive the ages. Consider these words from that day 77 years ago:
“We have come to a clear realization of the fact that true individual freedom cannot exist without economic security and independence.”
“Necessitous men are not free men. People who are hungry and out of a job are the stuff of which dictatorships are made.”
“In our day these economic truths have become accepted as self-evident. We have accepted, so to speak, a second Bill of Rights under which a new basis of security and prosperity can be established for all—regardless of station, race, or creed.”
“It is our duty now to begin to lay the plans and determine the strategy for the winning of a lasting peace and the establishment of an American standard of living higher than ever before known.”
“We cannot be content, no matter how high that general standard of living may be, if some fraction of our people—whether it be one-third or one-fifth or one-tenth—is ill-fed, ill-clothed, ill-housed, and insecure.”
“This Republic had its beginning, and grew to its present strength, under the protection of certain inalienable political rights…As our nation has grown in size and stature, however—as our industrial economy expanded—these political rights proved inadequate to assure us equality in the pursuit of happiness.”
In proposing this radical cultural shift, with war still waging across the globe but the tide clearly turning in the direction of the Allies, he defined those rights in black and white:
- The right to a useful and remunerative job in the industries or shops or farms or mines of the nation;
- The right to earn enough to provide adequate food and clothing and recreation;
- The right of every farmer to raise and sell his products at a return which will give him and his family a decent living;
- The right of every businessman, large and small, to trade in an atmosphere of freedom from unfair competition and domination by monopolies at home or abroad;
- The right of every family to a decent home;
- The right to adequate medical care and the opportunity to achieve and enjoy good health;
- The right to adequate protection from the economic fears of old age, sickness, accident, and unemployment;
- The right to a good education.
FDR loved America and all Americans. He rests in peace, but his words – and the promise they enshrine – have never died. They remain unfulfilled, their meaning and import reinforced on January 6, 2021 and beyond by the actions of insurrectionists, and anti-vaxxers, and political opportunists whose latest gambit is to sacrifice school children on an altar of profit and privilege.
President Biden shows signs of greatness, but must take care not to come up short – in voting rights, in national health care, in global warming. When dealing with determined and malevolent foes, words must be chosen carefully and delivered with absolute clarity.
“They are unanimous in their hate for me – and I welcome their hatred.”
Those were FDR’s words in 1936. Determined and deliberate. Defiant and dramatic. In defense of Democracy. This is the long awaited moment of truth for FDR, and President Biden.
The Unhealthy Leadership of Governor DeSantis.
Posted on | August 21, 2021 | 1 Comment
Mike Magee
On March 25, 1966, Rev. Martin Luther King Jr. said, “Of all the forms of inequality, injustice in health care is the most shocking and inhuman…”
This week, my niece in Orlando, Florida, sent her 8-year old son, masked, back to public school. He has a history of severe allergies, including several anaphylactic episodes requiring emergency respiratory intervention. His class included a voluntary mix of masked and unmasked children. He now has a 105 degree fever and has tested positive for the Delta variant of Covid.
His crisis, and those of countless other children in Republican led states, now lies clearly on their governors’ shoulders. It also suggests, as with voting rights, that we can no longer allow health planning and delivery to be captured entities of the states rights crowd. Dying children are just not acceptable in a civilized society.
The impassioned and illogical pleas of leaders like Florida Gov. Ron DeSantis are literally as old as this nation. As with many controversies in human endeavor, the easiest way to decipher history and meaning is often “to follow the money.” Such was the case in the battle between state and federal rights. This battle engaged early and often, with Thomas Jefferson and Alexander Hamilton on opposite sides of the spectrum.
Soon after the 1788 ratification of the U. S. Constitution, Washington’s Secretary of the Treasury, Hamilton, suggested a federal bank to manage debt and currency. Jefferson, then Secretary of State, opposed it for fear of a federal power grab. Regardless, in 1791, Congress created the First Bank of the United States with a 20-year charter.
When the charter ran out in 1811, it wasn’t renewed. But then the War of 1812 intervened, and in 1816 the Second Bank of the United States was created with the Federal government holding 20% of the equity. The divide reinforced the divide of two political parties – the Federalist Party and the Democratic-Republican Party whose members were committed to undermining the bank.
The battle came to a head when, in 1818, Maryland’s state legislature levied a $15,000 annual tax on all non-state banks. There was only one – the Second Bank of the United States, which refused to pay. The suit rose to the Supreme Court with Maryland claiming the right to tax based on their reading of the 10th Amendment claiming state protection against extension of non-enumerated rights to the Federal government.
The landmark 1819 case – McCulloch v. Maryland, defined the scope of the U.S. Congress’s legislative power and how it relates to the powers of American state legislatures. In ruling against Maryland, Chief Justice Marshall argued that:
“Let the end be legitimate, let it be within the scope of the constitution, and all means which are appropriate, which are plainly adapted to that end, which are not prohibited, but consist with the letter and spirit of the constitution, are constitutional.”
It was the people who ratified the Constitution and thus the people, not the states, who are sovereign.
One hundred and thirty years later, on December 10, 1948, the newly formed United Nations, adopted the Universal Declaration of Human Rights. That day, Eleanor Roosevelt spoke for America, stating: “Where after all do human rights begin? In small places close to home…Unless these rights have meaning there, they have little meaning anywhere.”
Of the rights enumerated and endorsed that day was included Article 25: Right to An Adequate Standard of Living. It read:
“Everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing, housing and medical care and necessary social services, and the right to security in the event of unemployment, sickness, disability, widowhood, old age or other lack of livelihood in circumstances beyond his control”, and “Motherhood and childhood are entitled to special care and assistance. All children, whether born in or out of wedlock, shall enjoy the same social protection.”
Professors like Jonathan Mann, director of the Health and Human Rights Center at Harvard School of Public Health, have added political heft to the debate. He agreed with a 2000 UN statement that “Health is a fundamental human right indispensable for the exercise of other human rights.” Why? He gives three reasons.
Political: “Health policies, programs, and practices have an affirmative impact on human rights, especially when state power is considered in the realm of public health.”
Discrimination: “Human rights violations have health impacts.”
A Propitious Cycle: “Protection and promotion of human rights and health are linked fundamentally in a dynamic relationship.”
What is somewhat remarkable is not what Professor Mann said, but rather how long it has taken to make its’ way from the streets of America to the ivy halls of academic, and now back again.
Covid, and its mutants and their enablers like DeSantis, are now part of our history. We the people, not the states, are sovereign. We must have the vote. We must protect our children. And we must have a national health plan based on science and truth.
Afghanistan, Covid, the Delta Variant …and Fear Management as a Public Health Emergency.
Posted on | August 17, 2021 | 3 Comments
Mike Magee
In the past two decades, all manners of catastrophe have managed to land on our laps at the intersection of science, public policy, and information technology. Transparency and truth are the keys to unlocking lasting solutions. But in the meantime, there is a pressing need to manage fear.
The U.S. evacuation from Afghanistan this week has simply added fuel to the fire. People are scared. And when people are scared, they not only make bad decisions, but they also make themselves sick.
It wasn’t too long ago that I tackled this very issue. The source point for the fear was different then: 9/11. I was charged to study fear levels in New Yorkers 30 months after 9/11 and again 4 years after 9/11.
The first study of 1,000 New Yorkers , 30 months post 9/11, disclosed high fear levels, especially with respect to using mass transit, and high residual levels of mental illness. It also noted that, while citizens were more vigilant, they did not see themselves in a position to contribute to a response to color coded warnings. In short, they absorbed the fear, but had little outlet for a constructive response. Four years post-9/11, fears over terrorism remained prevalent among New York City residents.
The suffering from mental ailments persisted as well. Thirty-five percent reported personally suffering depression, anxiety, or mental illness as a result of the 9/11 attacks. Fifty-two percent of those originally affected said they were still suffering from mental ailments. Of those who personally suffered, women, Hispanics and African Americans were disproportionately affected.
Our citizens reaction to Covid, and now the Delta variant, mirrors these findings.
Here is what I believe needs to be done:
1. Fear Management must become a core responsibility of those involved in Covid disaster response.
2. A mental health professional with strong public health credentials should be an active team member on local, state, and national levels.
3. All Covid recovery plans should include short, medium and long-term plans to manage fear and its mental health fallout.
4. Covid disaster communication plans, both proactive and reactive, should be rigorously focus tested to assess mental health impacts.
5. A comprehensive national public/private multi-media communication program to address residual fear head on and reinforce social confidence and trust in vaccines should be developed and launched.
What we must now recognize is that current fear left unaddressed and reinforced by frequent warnings and Delta induced flashbacks will not go away. It will persist, especially in the most vulnerable, and eat away at the fabric of society, eroding public confidence and trust in science and health professionals.
President Biden is doing his part, but he cannot do it alone. We together absorbed the fear. Together we must now confront and rid ourselves of it.
WSJ Denialists: “Same Climate Report, Different Day.”
Posted on | August 12, 2021 | Comments Off on WSJ Denialists: “Same Climate Report, Different Day.”
Mike Magee
This past weeks scary Climate Report raised alarm bells with good reason around the world. What’s not surprising is that the editorial page of the Wall Street Journal has not changed its tune. Holman W. Jenkins, Jr.’s headlined, “Same Climate Report, Different Day.” In some ways, he’s right – the finding (the News in the report) is actually not new.
In 1997, Gro Brundtland, then head of the WHO defined health as “human potential”. In doing so, she broadened the sphere of interest of health policy experts on a macro level and challenged physicians on a micro level. In essence she united for the first time patient health and planetary health.
Since that time, we have seen a continued battle and debate in the public space between the overwhelming majority of scientists who has raised the alarm over the self-reinforcing cycle of global warming, and a much smaller but highly vocal segment of the scientific community, who – often with the support of dollars from energy related corporations – have denied the challenge we and the planet face.
Exactly 7 years ago, in an article in JAMA, physicians for the first time were directly challenged to educate their patients regarding the coming health risks associated with global warming. The authors reviewed the evidence related to this impending crisis and come to this conclusion: “Evidence over the past 20 years indicates that climate change can be associated with adverse health outcomes. Health care professionals have an important role in understanding and communicating the related potential health concerns and the co-benefits from reducing greenhouse gas emissions.”
The article in part noted:
1. “Consensus is substantial that human behavior contributes to climate change: 97% of climatologists maintain that climate change is caused by human activities, particularly fossil fuel combustion and tropical deforestation.”
2. “About half of anthropogenic greenhouse gas emissions between 1750 and 2010 occurred since 1970. The increase in greenhouse gas emissions has been greatest in the last decade (2.2% per year) compared with 1.3% per year between 1970 and 2000.5 Emissions continue to increase; 2011 emissions exceeded those in 2005 by 43%.”
3. “Carbon dioxide from fossil fuels and industrial processes accounted for approximately 78% of the total increase from 1970-2010.”
4. “The trend toward decarbonization (cleaner fuels) of the world’s energy since the 1970s has been reversed by increased coal combustion since 2000.”
5. “Climate change is happening: the relationship of heat-waves, floods, and droughts along with adverse health outcomes is evident. Two broad approaches are needed to protect public health: mitigation, or major reductions in carbon emissions, corresponding to primary prevention; and adaptation, or steps to anticipate and reduce threats, corresponding to secondary prevention (or public health preparedness).”
6. Key health risks noted for doctors and patients included:
“Heat-related disorders, including heat stress and economic consequences of reduced work capacity.”
“Respiratory disorders, including those exacerbated by fine particulate pollutants, such as asthma and allergic diseases.”
“Infectious diseases, including vector borne diseases, such as Lyme disease, and water-borne diseases, such as childhood gastrointestinal diseases.”
“Food production, including reduced crop yields and an increase in plant diseases.”
“Mental health disorders such as post-traumatic stress disorder and depression that are associated with natural disasters.”
7. Mitigating climate change could yield health benefits:
“Economic advantages of reducing fossil fuel combustion and improving air quality, including a reduction in chronic diseases and their associated health care costs, and economic opportunities associated with development of alternative forms of energy.”
“Infrastructure improvements that reduce greenhouse emissions could also lead to increased physical activity that would be associated with a reduction in various chronic diseases.”
8. Heat related death and disability said the author, have been understated: “The most direct effect of a warming planet is heat stress and associated disorders. Heat-related deaths are routinely attributed to causes such as cardiac arrest without citing temperature as the underlying factor. Thus, the actual death toll attributable to heat is greater than certified on death certificates.”
9. Global warming will continue to reduce productivity: “Using industrial and military guidelines, Dunne et al estimated that ambient heat stress has reduced global population-weighted labor capacity by 10% in summer’s peak over the past few decades. Projected reduction may double by 2050 and may be even larger in the latter half of the 21st century.”
10. Additional death and disability secondary to food scarcity, respiratory disease and waterborne disease in all age groups and traumatic, disaster related injuries is to be expected. The mental health implications of these stressors are currently being underreported.
How can health professionals help?
“ Effective communication may shift knowledge, attitudes, and behavior toward reducing the risks of climate change. Research indicates several principles of effective climate communication that closely resemble those used in health. Themes include 2-way communication, gearing messages to the audience, limiting use of fear-based messages, issuing simple lucid messages repeated often from trusted sources, and making health-promoting choices easy and appealing.”
“Health may be a compelling frame for communication about climate change, reflecting views that change threatens health. Although further research is needed to define the role of health in climate communication, practical communication resources are becoming available, implying an important role for health care professionals.”
The WSJ’s Jenkins writes, “Corporate management has nothing material to add.” The 2014 JAMA article suggests that health professionals do.
« go back — keep looking »"Code Blue INDEX online"

![]()
![]()
Prospective Health Blog
BIOGRAPHY
NIH Precision Medicine
BIOGRAPHY
Health in 30
BIOGRAPHY
Larry's Letters
BIOGRAPHY
Precision Medicine, Euthanasia, Abortion, Communism, Trillions of Dollars, Losing Freedom, and Town Hall Mobs BIOGRAPHY
Yearning for Universal Coverage Is Not Universal
BIOGRAPHY

