Trump “Compstockery” – Militarizing Our Post Office!
Posted on | September 3, 2020 | 2 Comments

Mike Magee
As we witnessed in last month’s Republication convention, when in doubt, go with the golden oldies. Australian songwriter Peter Allen said as much in the fourth stanza of his classic song, “Everything Old Is New Again”, which reads:
“Don’t throw the past away
You might need it some rainy day
Dreams can come true again
When everything old is new again”
In fact, there’s nothing original in Trump’s playbook, and that includes his postal service gambit. Manipulating and militarizing the US Postal Service dates back to 1873 in the form of one Anthony Comstock, a zealot who was fond of describing himself as a “weeder in God’s garden.”
A savvy New York City insider, he created the New York Society for the Suppression of Vice declaring himself committed to stamping out smut. But to accomplish this task, he needed a hammer. He turned to political allies in the United States Postal Service who provided him with police powers and the right to carry a weapon.
Still, the weapon was of little use without a law to enforce. So he turned to his friends in industry who reached out to Congress. “An Act for the Suppression of Trade in, and Circulation of, Obscene Literature and Articles of Immoral Use” was passed on March 3, 1873, ch. 258, § 2, 17 Stat. 599. Forever after known as the Comstock Law, the statute’s lofty intent was “to prevent the mails from being used to corrupt the public morals.”
“Obscenity” was broadly described and included all print materials advancing birth control, abortion or family planning. Comstock held the post as special agent to the Postal Service for the next 42 years, and during that time bragged that he had prosecuted 3,600 defendants and destroying 160 tons of obscene literature.
In the face of Congressional failure back then, opposition among citizenry stiffened. There was Margaret Sanger who labeled Comstock a “moral eunuch” and edited “The Woman Rebel” whose motto was “Working Women, build up within yourselves a conscious fighting character against all things which enslave you.”
Sanger not only promoted family planning and women’s access to health care including abortions, but also challenged Comstock’s allies in industry writing, “We know the capitalist class must have a slave class, bred in poverty and reared in ignorance. That is why it is quite consistent with their laws that there should be a heavy penalty of five years’ imprisonment for imparting information as to the means of preventing conception. Industry…(must) undersell its rival competitors. They have only one way to do this, and that is to get labor cheap. The cheapest labor is that of women and children; the larger the number of children in a family, the earlier they enter the factory.”
Our nation then (and hopefully now) maintains the capacity to self-correct. In doing so, we rely on autocrats to over-play their hands. Trump is currently doing so with his face-off’s with LeBron James, Chris Webber and Doc Rivers.
A century ago, Comstock made poor choices as well. For example, he picked a fight with Irish playwright George Bernard Shaw by instigating the placement of his play “Man and Superman” on the “restricted book list” at the New York Public Library. Queried by the New York Times for his reaction to the affront, Shaw posted this response from London on September 25, 1905:
“Dear Sir – Nobody outside of America is likely to be in the least surprised. Comstockery is the world’s standing joke at the expense of the United States. Europe likes to hear of such things. It confirms the deep-seated conviction of the Old World that America is a provincial place, a second-rate country-town civilization after all.”
Ouch!
The Supreme Court upheld the Comstock Law until 1983. In Bolger v. Youngs Drug Products Corp., 463 U.S. 60, 103 S. Ct. 2875, 77 L. Ed. 2d 469 (1983), the Supreme Court re-examined the Comstock Law and concluded it did not support “a substantial governmental interest.” In an historic smack down the Court declared, “that a restriction of this scope is more extensive than the Constitution permits, for the government may not reduce the adult population … to reading only what is fit for children.“
____________________________________________________________________________
Originally Published: The Health Care Blog/Sept. 1, 2020
Tags: Comstock > Health Care Fraud > Maternal Health > trump > US Postal Service > Womens Rights
Americans Need To Stay Well To Get Better.
Posted on | August 27, 2020 | Comments Off on Americans Need To Stay Well To Get Better.
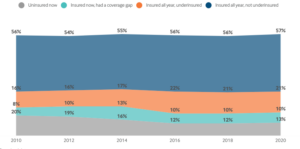
Source: Commonwealth Fund 2020 Insurance Study
Mike Magee
In the face of the covid-19 rolling disaster, Americans without adequate health insurance are now closing in on 50%.
Relying on employers to provide health insurance has always been a bad idea. Lose your job/lose your insurance is crazy. That’s why no other developed nations go for it. As Warren Buffett says, its the “tapeworm on America’s economic competititiveness” restricting job mobility, productivity and efficiencies at every turn.
According to the recently released Commonwealth Fund study, in the first six months of this year, 12.5% of Americans lacked any insurance and another 10% had a period of absent coverage (a coverage gap). But what’s worse is that 21% were demonstrably underinsured – lacking basic benefits and hobbled by high deductibles and crippling copayments.
Over the past decade, many employers have purposefully shifted the financial risk to employees and with stealth degraded their offerings. Fully one quarter of all employers providing health coverage purposefully “under-insure.” Back in 2010, only 7% of plans had deductibles of 5% or more of their income. Now it’s above 15%. In 2010, 22% elected plans with base deductibles of $1000 or more. Now it’s a startling 46%.
Even before the pandemic – with its huge rates of unemployment and increases in mortality and morbidity – Americans couldn’t pay their health care bills. One in four with a job were dogged by medical debt. For the uninsured and underinsured, it was one in two.
As the pandemic hit, Americans tightened their belts, and checked their savings. But 37% said they had used up all their savings to pay their bills. Medical debt had already tarnished the credit ratings of 40% of Americans.
As Trump fiddles, and the pandemic spreads out-of-control, a quarter of our citizens already report problems paying for the basics – like food, medicines, and rent. With federal relief packages now in limbo, and the cold weather arriving (bringing seasonal flu into the mix), it becomes clear we are vulnerable as a nation.
There’s much to do. But none of it can be done if the citizenry is sick or disabled. We need to stay well to get better. And no one understands that better than employers. They need to come clean and simply say out loud, “We want out of the health care business.”
Open Source and Worth Sharing: A Jesuit Perspective – “Contemplating U.S. Health Care After Covid-19”
Posted on | August 24, 2020 | Comments Off on Open Source and Worth Sharing: A Jesuit Perspective – “Contemplating U.S. Health Care After Covid-19”
“Show Me State” Abandons Trumpian Orbit and Embraces Medicaid Expansion.
Posted on | August 18, 2020 | 4 Comments
Mike Magee
Idaho
Utah
Oklahoma
Nebraska
Maine
…..
(and now) Missouri.
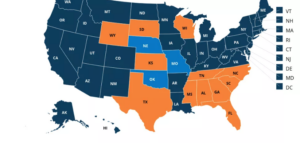
Since 2017, six Republican-led states have buckled under the crippling costs of health care and embraced the ACA offer to subsidize expanded Medicaid coverage for vulnerable populations in their states.
The “Show Me State” showed its defiance and hard-heartedness until their state budget bled bright red in response to mismanagement of the Covid-19 pandemic. The final reversal came in earshot of Trump’s musings to Chris Wallace on FOX about a “health-care plan within two weeks, a full and complete health-care plan” and laughable pledges to “repeal Obamacare” just as 45 million additional Americans became unemployed and uninsured simultaneously.
By 6%, Missourians voted to extend health coverage to an additional 200,000 state dwellers. Those votes came dramatically from former Trump leaning suburbians. Even the state’s rural voters are beginning to get the message, having seen 10 rural hospitals shut their doors in the past few years.
Twelve hold-out states remain – 8 of the 12 from the Old South. That leaves some 2 million vulnerable citizens without coverage that is readily available. Polls in those states show that 2/3rds of their citizens favor Medicaid expansion in opposition to their own governors – and that was before the pandemic. Even in red counties of red states, 1/3 of Republicans are polling in favor of Medicaid expansion.
Democratic politicians like Montana Senate candidate Steve Bullock are running with the news. He’s up on the air promoting state expansion of Medicaid to benefit “rural hospitals all across Montana.”
Who’s next? All eyes are on Florida and its 2.7 million uninsured residents.
Is This Seasonal Flu or Covid-19?
Posted on | August 14, 2020 | 2 Comments

Mike Magee
“Is this seasonal flu or Covid-19?” That’s the question many doctors and patients hope to avoid this fall.
Here are three strategies designed to avoid panic and even greater disruption of individuals lives and malfunction of our already over-stressed health care system:
Strategy 1: Get Your Flu Shot Early.
Approximately 200 million flu vaccine doses have already begun to hit the market in the U.S. This is a 20% increase over last year and presumes an above-normal demand for the preventitive inoculation. AstraZenca has already released its first shipment of their FluMist vaccine after bumping up its original production by 25%.
Strategy 2: Dual Testing for Flu and Covid-19.
Last month the FDA approved a joint COVID-19 and flu test. This potentially will arm health professionals with a tool to avoid the either/or dilemma that faces them just around the corner.“With the authorization of these tests, the FDA is helping address concerns in anticipation of this upcoming flu season during the COVID-19 pandemic, which might be especially worrying for some Americans” said FDA Commissioner Stephen M. Hahn .
Strategy 3: Target vulnerable populations
In early June, with Trump undercutting infectious disease risk at every turn, the CDC gave $140 million to 64 localities to help states prepare for the flu season. By targeting an increase in flu vaccinations for vulnerable populations and increasing access for uninsured, high-risk people, the agency believes it will achieve a multiplying effect – decreasing hospitalizations for both flu and COVID-19.
Experts at the Institute for Health Metrics and Evaluation now predict over 300,000 U.S. deaths from COVID-19 by December accompanied by a 75% increase in hospitalizations over the next 3 months due to Trump’s encouragement of lax policies for containment. Even if defeated in November, Trump is signaling his intention to spend his last two months in office further complicating and undermining a “good government” response to this health and economic catastrophe.
This leaves control mesures in the hands of local leaders, health care professionals and patients. Three things you can do: 1) VOTE, 2) Mask and distance, 3) Get your Flu vaccine early.
The Origin Story of PBM’s.
Posted on | August 13, 2020 | 2 Comments
Mike Magee
Do you know the origin story of PBMs, and why they and their middlemen hold 6 of the top 25 spots in the Fortune 500? Here’s a starter course, excerpted from “CODE BLUE: Inside the Medical Industrial Complex” where the full answer resides.
“When PBMs began, insurers and employers believed that this new entity might contribute to cost control by efficiently processing prescriptions, maintaining approved drug formularies, and holding down prices. But they soon realized that ownership of a PBM by a drug-maker, insurer, or a retail pharmacy giant allowed the owner to coordinate pricing decisions, see competitors’ pricing information, and favor some drugs over others in return for kickback payments, even if the consumer unknowingly was forced to pay more.
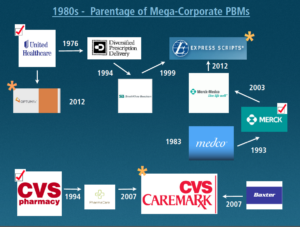
There are now about thirty different PBMs. But three major companies control 78 percent of the PBM market and service 180 million Americans.61 These opportunistic middlemen emerged from three different Medical Industrial Complex (MIC) industry sectors: a physician managed care group, a pharmacy corporation, and a pharmaceutical manufacturing company.
The first one, Diversified Prescription Delivery, was developed in 1988 by UnitedHealthcare, the insurance company that grew out of a physician-run managed care medical group called Charter Med, incorporated in 1974. They were the first to recognize that new information technology would revolutionize the health care industry. Where the WHO owned the ICD-9 diagnosis billing code databases, and the AMA owned the CPT procedure billing code databases, UnitedHealthcare ambitions were far more expansive–to control and mine patient databases themselves. From this perch, they were the first to develop pharmacy drug formularies, hospital admission pre-certification requirements, physician office software that predated electronic medical records, and tight controls on utilization beyond those of other HMO’s at the time.61
The realization that data now was king spread rapidly. A second PBM, PharmaCare, appeared as an offering from CVS in 1994, and in 2007 was renamed CVS-Caremark.62 The third dominant PBM, mail order giant Express Scripts, has a complex parentage. It was formed from the purchase of a SmithKline Beecham’s PBM in 1999 and the addition of Merck-Medco in 2012.63 Five years later, in 2017, Express Scripts reported revenue of over $100 billion compared with Pfizer’s $52 billion of revenue that year.64
Their sphere of influence and market power derives from the fact that approximately 4.5 billion prescriptions are filled in the US each year. Americans’ appetite for legal drugs is close to insatiable. Just under 50 percent of US residents have filled a prescription in the last month, and 10 percent of our population currently takes five or more prescription medications.

Approximately $50 billion is expended each year in the manufacturing of these drugs, which move primarily through three giant wholesale distributors in the US—AmerisourceBergen, Cardinal Health, and McKesson—on their way to the retail pharmacy. Their combined revenue in 2015 was $378 billion for distributing the drugs to 60,000 pharmacy outlets, 63 percent of which are part of large retail chains. By 2017, their combined revenue reached $481 billion.65
PBMs are now the Grand Central Station of the legal trade of drugs and the primary processors of patient and insurance enrollee data. They negotiate the deals for each and every drug with pharmaceutical companies, the placement of those drugs on insurers’ and employers’ tiered insurer formulary drug lists, and the integration and management of utilization and cost strategies with pharmacies, insurers, and hospitals nationwide. Their cutouts and givebacks to both the drug and insurance industries, and negotiations with hospital systems, share the profits and are nontransparent. Nearly everyone is in on the deal—except the patient.”
Tags: AmerisourceBergen > CardinalHealth > CVS Caremark > Express Scripts > health cost > health fraud > health reform > McKesson > MIC > Optum > PBM
A Marshall Plan For America
Posted on | July 30, 2020 | 7 Comments

Mike Magee
Yesterday close to 300 registrants signed up for a webinar sponsored by my Jesuit alma mater, LeMoyne College, titled “The Birth of the Medical Industrial Complex in America, and How Covid-19 Has Made the Case For a National Health Care System”. The college’s motto, “Greatness meets Goodness”, speaks highly of their value system, especially during these challenging times.
During the one hour Zoom presentation, questions flowed in over the chat line which you’ll see reflected in future posts. But the first question asked was, “What do you feel is the most important action step that needs to be taken to start enacting wide-spread change?”
My answer was, “Vote in November.”
I followed that quick response with what I would describe as “A Marshall Plan for America.”
During the presentation, I had shared the fact that, as America’s burgeoning Medical Industrial Complex coalesced in 1950 to beat back President Truman’s plans for a national health care system for our citizens, American taxpayer dollars financed the Marshall Plan construction of national health systems for our two vanquished enemies, Germany and Japan.

In a Rand Corporation post-mortem on nation building some decades later, scholars remarked that, “Nation-building efforts cannot be successful unless adequate attention is paid to the health of the population.”
In the re-build of Germany and Japan under the Marshall Plan, we elected to start with a health plan – in part because we recognized that all other social determinants – justice, housing, nutrition, education, clean air and water, transportation, safety and security – would be enhanced in the process.
We understood that this 1948 infusion of what would today amount to $128 billion would engender trust, improve health and productivity, and process fear and worry which might otherwise undermine the establishment of a civil society and stable democracy.
In answering yesterday’s question, I suggested that we as American citizens essentially face a challenge of similar magnitude.
In rejecting Trump, we are battling the dual scourges of a badly mismanaged pandemic response and the fires of historic and systemic racism. But in addition, we are opening the doors to a cultural and political awakening that could be “A Marshall Plan for America.”
The health care underpinnings of such a plan were driven deep into our cultural soil over a decade ago and have survived relentless attempts to unearth and destroy. These include fundamentals: Health is essential and a universal right. Universal health coverage is necessary to assure population health. All health plans must include comprehensive benefits. Patients with pre-existing conditions must be protected. Our most vulnerable populations are a top priority.
Upon these anchors, and now the sacrifices of over 150,000 Americans dead in part because of Trump’s incompetence, we see revealed the basic “next-step” building blocks of a new deal for America.
Universality: Coverage for all – shared responsibility and risk.
Strategic Planning: Multi-year national health priorities layed out by a truly representative governance body.
Efficiency: Streamline payments, annual negotiated budgets, strict oversight, standardized national billing and payment systems.
Transparency: No DTC advertising. No kickbacks inside PBM’s. No data profiteering. Industry funded academic researchers must register as lobbyists.
Local Control of Delivery: Federal standards with local autonomy. Public insurance is primary. Private insurers are secondary and supplemental.
The unleashing of a Marshall Plan for America could be triggered by the offering of a “public option.” The response of parents of adult children, employees on skimpy employer based plans, newly covid unemployed, underinsured, uninsured and vulnerable will further strengthen our national resolve and advance our evolution towards unification, peace and productivity.
As Trump and Covid have made clear, “a thousand points of light” is no more a substitute for “good government” than it was for our vanquished enemies following World War II. As we did for them then, we must now ask the difficult question “How do we make America, and all Americans healthy?”
And then build out the answer – from the bottom up.
"Code Blue INDEX online"

![]()
![]()
Prospective Health Blog
BIOGRAPHY
NIH Precision Medicine
BIOGRAPHY
Health in 30
BIOGRAPHY
Larry's Letters
BIOGRAPHY
Precision Medicine, Euthanasia, Abortion, Communism, Trillions of Dollars, Losing Freedom, and Town Hall Mobs BIOGRAPHY
Yearning for Universal Coverage Is Not Universal
BIOGRAPHY

