What Friedman and Sandel and Desmond (and Maine) Know About Our Nation’s Health.
Posted on | November 7, 2017 | 4 Comments
Niger and Waco
Mike Magee
We wake this morning to news that Maine voters have overrode their own governor and expanded ACA Medicaid, and Virginia voters have rejected a Trumpian appeal. As we begin to turn the corner, we need to be certain we don’t simply return to neutral but instead understand and execute progress. Health policy is the ideal catalyst.
When it comes to policy matters (whether they be related to taxes, or guns, or advertising), Canada historically has exhibited great natural instincts and a healthy dose of holistic common sense.
Consider the fact that at the end of WWII, with veterans streaming back into the country weighed down with a heavy burden of diseases, addictions, and psychiatric disabilities, Canadian leaders realized that the success of their country ultimately would depend on the health of Canadians. They wisely saw health as a human right, and realized that lack of coordinate health planning coupled with excessive free marketering would drive up cost and complexity, placing an undue burden on all of their citizens.
Compared to Canada which chose universality and simplicity, following WW II we elected to stay mired to individualism and “free enterprise” approaches reasoning that if we could beat the Nazis, we could easily beat disease, and health would thrive in its wake.
The results of this unending experiment have been singularly disappointing. Scientific progress has become unlinked from human progress. One in five dollars is now committed to a speculative Medical-Industrial Complex that continues to grow in size and appetite. And the gap between have’s and have-nots leaves a gaping hole in our national stability, optimism, and civility.
Our failures in the health sector increasingly draw comparisons to developing nations rather than to our historic developed peer nations. Fundamentally, we seem so infatuated with discovery, patents, and corporatized solutions that we manage to silently deny that health is a function primarily of social determinants.
Tom Friedman understands this. He recently focused on the struggles in Niger which came under a glaring spotlight when we lost four U.S. Special Forces in a battlefield that most Americans didn’t know existed.
Friedman wisely focused not on the losses, as tragic as they were, or even the conflict itself, but on the underlying causes. The destabilization of this region in Africa and the explosion of “economic migrants, interethnic conflicts and extremism” is tied to the ever “widening collapse of small-scale farming”. That collapse, in turn, is a function of four intersecting triggers – climate change, Saharan desertification, population explosion (Niger’s birthrate is 7.6 children per woman), and misgovernance.
In light of the above, how does America’s president respond beyond putting our soldiers at risk? By eliminating U.S. support for global contraceptive programs; by supporting climate deniers; by pushing exportation of coal to Africa; and by curbing climate research.
It would be easy to suggest that Trump is an outlier, but as we hot-tail it to “personalized medicine” and stem cell this and that (all good but speculative and of little impact on immediate population health), we way miss the forest from the public health trees.
For example, Megan Sandel and Matthew Desmond this week laid out the connection between health and housing. But was anyone but John Kasich listening?
A few facts:
1. In America, “2.8 million renting households are at risk of eviction and more than 500 000 people are homeless on any single night.”
2. “Only 1 in 4 households that qualify for housing assistance receives it… most renting households below the federal poverty line spend more than half of their income on housing costs, and 1 in 4 spends more than 70% of its income on rent and utility costs alone.”
3. “Rent-burdened families not only have less money to spend on wellness and health care but also regularly face eviction and homelessness, which further threaten their health.”
4. “Housing problems have been associated with a wide array of health complications, including lead exposure and toxic effects, asthma, and depression.”
5. “The top 5% of hospital users—overwhelmingly poor and housing insecure—are estimated to consume 50% of health care costs.”
6. “Randomized trials have found that hospital stays and emergency department visits decreased among homeless individuals after they were offered stable housing and case management.”
The authors conclusions:
Friedman: “ Nothing Trump ever says has a second paragraph. His whole shtick is just a first paragraph: Build a wall, tear up the Iran deal, tear up TPP, defeat ISIS, send troops to Niger and Afghanistan to kill terrorists, kill climate policy, kill family planning, cut taxes, raise military spending. Every box just marks an applause line he needed somewhere to get elected. Nothing connects — and we will pay for that.”
Sandel and Desmond: “ A stable home functions as a secure foundation on which to build holistic and cost-effective health care. Without this foundation, medical treatments are reduced to short-term, limited fixes that must be applied and reapplied at significant cost and insignificant health gains. Hospitals and health systems can and must do better in investing in homes for health, for both patients and the broader community.”
And Kasich, to a major GOP donor who challenged his support of Medicaid expansion in Ohio at a Koch brothers conference: “I don’t know about you, lady, but when I get to the pearly gates, I’m going to have an answer for what I’ve done for the poor.”
Tags: health and housing > health policy > JAMA > John Kasich > Niger > NYT > public heal > Social determinants of health > Thomas Friedman
Disrupter in Chief – CVS, Aetna, or Amazon?
Posted on | October 30, 2017 | 3 Comments

Mike Magee
In 1964, a purveyor of general merchandise based in Rhode Island, coalesced 17 locations under one entity. They were focused on market data, inventory management, and economy of scale. Within five years, they were successful enough to have 40 locations, three with in-store pharmacies.
Within another decade, they had standardized their information, data, and business systems, and their annual sales had long exceeded $100 million. By 1985, they topped $1 billion. They now have 9,700 stores and in 2016 generated over $200 billion in revenue with 60% coming from pharmacy services. Their original name was Consumer Value Stores, but now everyone just calls them CVS, the seventh biggest corporation by revenue in the United States.
You might say they were the original disrupters in health care. And they’ve tried to keep their eye on the ball. For example, they’ve known that internet sales were a threat to their retail non-drug sales. Three years ago, in-store general purchases made up 52% of their revenue. Now it’s only 46% and continues to drift south. In response, they’ve looked at the lucrative U.S. pharmaceutical 4.5 billion prescriptions per year market worth $560 billion a year for every conceivable angle.
Some years back, CVS tip-toed into the provider space with their in-store Minute Clinics. That’s been a partial success. In 2007, they purchased Caremark, a pharmacy benefit manager, to capture supply chain management revenue, and that’s been good. They signed up insurer Aetna to a 12-year PBM contract in 2010. They’ve thought about more horizontal expansion – more stores – but the federal government rejected a bid by their arch rival Walgreen when it attempted to merge with Rite-Aid drugs, viewing it through an anti-trust lens. The feds did the same thing in blocking two different attempts by health insurers to merge last year.
For CVS, it’s been difficult to sit still and watch others go vertical. Take UnitedHealth Group, the insurance giant started by a physician, which now also owns its own PBM under the health services banner, Optum. They’re doing great with 3rd quarter earnings up 26%. Then there’s Anthem, the BC/BS insurer, that got in a nasty fight with their former ally, stand-alone PBM, ExpressScripts. Now Anthem is also starting its’ own PBM. Together Caremark, Optum and ExpressScripts control 80% of the PBM market.
Four months ago, health analyst Robert Flynn pointed CVS in the vertical integration direction, providing six reasons why he thought they ought to buy insurer Aetna with access to their 22 million customers. The reasons included that horizontal merger consolidation options were no longer feasible; competitors like United-OptumRx were gaining traction; the risk would be low since Aetna was already a Caremark customer; it would beat Express Scripts to the punch either as an insurance purchaser themselves or alternately being purchased by Walgreens; and the vertically oriented CVS-Caremark-Aetna goliath would be in a good position to do value-based contracts – like those advanced for Hepatitis-C cures.
So with this kind of forecasting, it shouldn’t have been big news last week when CVS and Aetna announced that negotiations for a CVS $66 billion buy-out of Aetna was underway. Their combined valuation would exceed $240 billion. But strangely enough, the original health disrupter in chief was out-disrupted by the ultimate disrupter of all, Amazon.
The New York Times headline said it all – “CVS and Aetna Talks Take Place Under Amazon’s Shadow.” What triggered this take-down was a new report in the St. Louis Post-Dispatch a day earlier that Amazon had won approval for wholesale pharmacy licenses in 12 states (NV,AZ,ND,LA,AL,NJ,MI,CT,ID,NH,OR,TN).
 “There are a lot of differences between books and drugstores, but there are a lot of similarities, too. Customers want selection, convenience, price and information.” Jeff Bezos, Amazon CEO
“There are a lot of differences between books and drugstores, but there are a lot of similarities, too. Customers want selection, convenience, price and information.” Jeff Bezos, Amazon CEO
The stories trumpeted Amazon’s market cap of $524 billion, and their history of upending other sectors like cloud computing, logistics and groceries. Marketing professors like Scott Galloway of NYU turned to florid prose. His prediction: “You will see strange bedfellows. P&G and Unilever, Nike and Adidas are going to come to the realization that they are competitors, not enemies. Their real enemy is in Seattle. When German tanks rolled into Slovakia and Poland, the Russians, British and Americans found a way to get along. The tanks {Amazon} have rolled in.”
CVS CEO Larry Merlo didn’t seem phased. He said, “We’ve seen threats in the past, OK.” He’s presuming that health care is different, too complicated for Amazon. But complexity is the pay-dirt that could bring success out of failure. Consider this model transaction as it exists today:
Original Stream:
Step 1: Pharma Company sets a price of $100 as the list price for 30 day supply of XYZ pill.
Step 2: Pharma Company marks-up the wholesale price to $110 and sells to one of three giant national wholesalers (McKesson, Cardinal, AmerisourceBergen).
Step 3. Wholesaler bumps price to $120 and sells to pharmacies.
Step 4. Pharmacy marks the price up to $130.
Secondary Back-Stream:
Step 5. Insurer Pays PBM $140 but receives a $45 rebate from the PBM. (Net payment by insurer is $95.)
Step 6. That $45 payment to the insurer came from a $50 rebate from the Pharma company. PBM keeps $5 of the rebate for itself. (Pharma profit: $110 -$50 = $60)
Step 7. PBM pays $110 and patient co-pays $20 to the pharmacy. (Pharmacy keeps $10.)
Step 8. PBM nets $35 profit. (Difference between $140 from insurer, and sale to pharmacy/patient for $110, plus $5 from Pharma’s $50 rebate)
You think Amazon might be able to figure out how to skip a few of these steps – like the wholesaler and the retailer and the PBM? And that doesn’t even consider the possibility that Seattle and Washington, D.C. might discover each other along the way.
Tags: amazon > Caremark > cvs > CVS Aetna merger > drug costs > drug rebates > Express Scripts > Optum > UnitedHealth
Single Payer Health Reform – A Solution For U.S. Income Inequality?
Posted on | October 26, 2017 | Comments Off on Single Payer Health Reform – A Solution For U.S. Income Inequality?
Mike Magee
Veteran Health Policy expert, James A. Morone, Ph.D., makes an interesting argument for single payer health care in this week’s NEJM. In proposing a sweeping change that would directly address “the American patchwork”, assert “the norms of communal decency”, promote planning and efficiency, and empower “a righteous band of reformers, deeply committed to a cause, pushing against all odds”, he does not sidestep higher taxes on the rich.
Rather he sells into them, presenting high taxes on the rich in return for universal health coverage as “on a short list of available policies designed to push back on inequality.
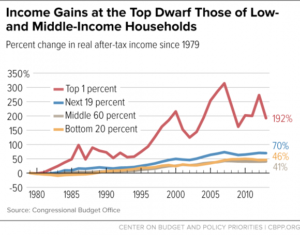
His argument boils down to the fact that a certral element of the national crisis we call “Trump” is populist anger grounded in remarkable income inequality. In roughly a half-century, our separation between rich and poor which used to mirror France and Japan, now aligns with Mexico and Brazil.
In short, we’re a mess, and our citizens are pretty fed up. And why shouldn’t they be? Our top 1% controls roughly 40% of all wealth, while the bottom 90% manages a paltry 23%. If you’re a white family in America, you were born lucky. On avaerage, your family is about 10 times as wealthy as your black family counterpart.
But what about taxes, and distrust of “Big Government”? Morone reminds us that major policy changes can, and have, flipped on a dime in the past. As he says, “Disruptive populism ended past American gilded ages, and it shows signs of challenging the current one.” With better health delivery, and more equality and social justice, we might also redirect the course of American politics and American politicians.
In the same issue of NEJM this week, Henry J. Aaron, Ph.D., explores different roads to reform, raising legitimate concerns about the unintended consequences of disrupting existing insurance holders, and arguing for a more cautious incremental approach including extending availability of Medicare and Medicaid to others, and shoring up ACA exchanges. He wonders how far and how fast are Americans willing to go?
This week, New York Times columnist, Thomas Friedman, shared his view. He didn’t pull punches when he accused Trump of intentionally undermining the two critical pillars of American society, truth and trust.
Interestingly, in the careful analysis of these two health policy experts above, both identify an embattled and epic American struggle over how to topple the health care status-quo, a Medical-Industrial Complex controlled and directed by members of the 1%, and a debate that currently hangs on whether we – the citizens – are able to discern fact from fiction.
The key question for health reform and for the future of America: Do we trust a government “of, by, and for the people” to assure that each of its citizens has the right to “life, liberty, and the pursuit of happiness?”
If a majority of us can move to “yes” on that question, we will find a way to embrace each other equally through health reform. And the quality and durability of that embrace will be determined by these Code Blue principles:
1. Universality: Health coverage is a right of citizenship.
2. Public Administration: Administration of basic health coverage is organized in the most cost-efficient manner possible with central oversight by the government.
3. Local Control of Delivery: The actual delivery of services is provided by health professionals and hospitals at the local and state levels.
4. Health Planning is a Priority: Creating healthy populations is a high priority on the federal and state levels.
5. Transparency: Providers submit bills. Government ensures payment of bills. Patients focus on wellness or recovery.
Tags: health care a right > health care reform > Henry J. Aaron > James A. Morone > NEJM > single payer > Thomas Friedman > universal health care
Why are cigarette smokers congregating in Unhealthy States?
Posted on | October 23, 2017 | Comments Off on Why are cigarette smokers congregating in Unhealthy States?


Will Rogers on Fellow Okie, Scott Pruitt.
Posted on | October 17, 2017 | Comments Off on Will Rogers on Fellow Okie, Scott Pruitt.

Mike Magee
Oklahoma’s favorite son, Will Rogers, once said, “Live in such a way that you would not be ashamed to sell your parrot to the town gossip.”
On August 2, 2017, that parrot was doing overtime, and he kept squawking, “Pruitt, Pruitt, Pruitt.” That’s because Oklahoma had just experienced 7 earthquakes in 28 hours. Scientists agree that these increasingly common geological events, rare in the state until 2009, are the result of injecting heavily contaminated fracking wastewater in underground disposal wells.
Adding insult to injury is President Trump’s appointment of former Okie attorney general, Scott Pruitt, as head of our nation’s Environmental Protection Agency. That’s the very same agency to which he had mailed a letter requesting regulatory relief using exact oil company text cut and pasted onto his official state stationary. That little offense was after he had challenged core results of climate scientists on global warming, and after he sued the EPA for relief from having to enforce regional smog rules including levels of airborne mercury pollution.
Not only did Oklahoma frackers inject their own wastewater, but they had been happily importing other firms wastewater for disposal after states like Kansas and Arkansas began restricting the practice. In 2015, this amounted to an additional 2.4 million barrels of the stuff, imported and injected into Oklahoma’s subterranean landscape.
 Source: YouTube
Source: YouTubeBut not surprisingly, this was pretty good politics. Pruitt’s campaign manager was oil billionaire, Harold Hamm, who notoriously stated at the Republican National Convention in 2016, “Every time we can’t drill a well in America, terrorism is being funded. Every onerous regulation puts American lives at risk.”
Pruitt and Hamm’s situational ethics aside, evidence is mounting that there is more for Okie citizens to worry about than just a few broken dishes. What they are playing with in Okie health.
1. More than half of our domestically consumed oil and gas comes from fracking.
2. The process involves injecting high pressure, treated water into porous rock strata accessed through horizontal well drilling. Over 100,000 domestic wells have been drilled in the past decade.
3. Ten states sit over vast shale depots including Pennsylvania, New York, Ohio, Maryland, Virginia, West Virginia, Kentucky, North Dakota and Montana.
4. Fracking is complex, multi-stepped, and carries proven risks of air, soil, and water pollution.
5. The water injected during fracking includes sand and a range of chemicals including silicates, acids, and surfactants. The wastewater recovered is contamininated with heavy metals like barium, manganese and iron, radium, and organic compounds lincluding benzene, toluene, xylenes, oil and grease. 95% of that wastewater is injected into deep disposal wells underground.
This week’s JAMA report outlined a range of health concerns including:
1. Asthma: In the states overlying the Marcellus shale (Pennsylvania, New York, Ohio, Maryland, Virginia, West Virginia, Kentucky), asthma patients living near wells were more likely to fill a prescription for oral corticosteroids than control patients living farther away.
2. Silicosis: Workers now must be monitored longitudinally to measure the impact of their respiratory exposure to crystalline silica.
3. Studies are now looking at both neurotoxicity and nephrotoxicity of fracking effluent. This includes manganese impact on basal ganglia and potential association with parkinsonism, mercury effects on dorsal root ganglia and association with idiopathic neuropathy, conversion of mercury to the more toxic methyl mercury by aquatic microorganisms, and altered renal function in those exposed to fracking water.
EPA head Scott Pruitt spends a great deal of time these days flying around on private jets at taxpayers expense. But he’d do well to spend more time on the ground with eyes wide open. Here are a few things he might look to regulating:
1. Fracking fluid spills.
2. Fracking storage wells wells with sub-par mechanical integrity.
3. Injection of fracking fluid into ground drinking water.
4. Inadequate treatment of fracking effluents.
5. Disposal of fracking fluid into unlined and permeable pits.
Or as Will Rogers said, “When you find yourself in a hole, quit digging.”
Tags: earthquakes > EPA > fracking > fracking fluid > Oklahoma > Scott Pruitt > Will Rodgers
The Catholic Playbook on Contraception, Circa 1950…and The Doctor’s Role In It.
Posted on | October 10, 2017 | 1 Comment
A Little Sister & Friend
Mike Magee
Who knew – The Little Sisters of the Poor’s new best friend would be Donald Trump?
Catholic institutions were first in line to challenge the ACA, followed by a motley crew of Obama haters who persisted for two terms before being exposed as having no legitimate health policy alternative. And now the Trump administration says they don’t have to obey Obama era rules in their organizations and cover contraceptive costs for their employees.
For anyone who has followed the Catholic Church’s embrace of birth control as a defining issue over the past 100 years, the Little Sisters benign expressions married with legal tactics should come as no surprise.
I know whence I speak. My doctor father inherited his mother’s devotion to the Catholic Church. Returning from WW II, he embraced the rituals and the sacraments. He would sink into deep contemplation at Sunday mass each week. And he loved being the selected doctor to the priests and nuns of the parish. My mother loved the structure and the concrete set of rules and beliefs that provided a scaffold and creed to build a life around.
Together they were a model Catholic family of the 1950’s – he a Catholic doctor serving mostly 1st generation Catholic immigrants, and she the mother of twelve Catholic kids.
As war veterans were returning, and the baby boom igniting, the Catholic Church doubled down on its ban of contraception. Science had progressed during the 1940’s and the basic understanding of fertility and manipulation of the ovulatory cycle had arrived.
The American Catholic Church and its’ leadership could easily predict the next step. It was only a matter of time before pharmaceutical companies and their allied physicians would figure out how to manipulate and destroy this miraculous system. Clearly, God’s right to decide when and where to deliver His children was under attack, and the Church must defend, defend, defend.
As Pope Pius XI had said in his famous Encyclical, Casti Connubi, on December 31, 1930: “…every attempt of either husband or wife in the performance of the conjugal act or in the development of its natural consequences which aims at depriving it of its inherent force and hinders the procreation of new life is immoral; and that no ‘indication’ or need can convert an act which is intrinsically immoral into a moral and lawful one.”
With modernity crushing in from all sides, the Church decided to embrace what was essentially a defensive move – the new “Rhythm Method” which at least emphasized restraint and periodic abstinence, and might dampen the march toward use of horrid preventatives, paganism, and sins of the flesh.
But who would teach and proselytize this new method which combined temperature based predictions of ovulation and fertility with voluntary abstinence? The answer was Catholic doctors like my father.
![]()
![]()
The vehicle the Church selected to deliver instruction on Catholic family planning was described thoroughly in the Archdiocese of Chicago’s 203 page book entitled The Basic Cana Manual. Cana and Pre-Cana Conferences were designed to be lay led meetings, with parish priest in attendance, focused on both marriage preparation and marriage renewal. My parents, as selected lay leaders, beginning in 1949, read the book from cover to cover, and participated as leaders in delivering the messages.
For them, it was a night out, free of the children; an opportunity to enjoy each other’s company, and to perform “on stage” which was a shared interest. They were not particularly worried or concerned about the dogma, or communicating the fear piece well. Sin and hell were not really their thing, any more than the “Sister is always right” mentality of most Catholic parents who sent their kids to Catholic schools. Their major mutual interest was in marital love and fidelity, the joy of commitment in good times and bad, and the rewarding challenges of managing very large families.
In any case, they found a lot to like in The Basic Cana Manual. The words on page 3, penned by the Reverend Walter J. Imbiorski, who presumably was chaste and celibate, struck a realistic and empathetic tone. “We fall in love and we get married and presently disenchantment sets in, the sense of adventure leaves us. And even this is no particular surprise. Doesn’t it happen to everybody? We share, day after day, all that goes into the common effort, the continuing adventure, of establishing and sustaining a family. But what does it add up to? We go through all the motions of marriage, but how involved are we?…Cana is dedicated to restoring that poetry which is the Divine idea of man and woman and marriage. Cana is really a meditation on man and woman and all that is implied in the words ‘one flesh’.” And a few sentences later, the smooth and gentle segue, “Once reverence for the supreme wisdom of the Creator of nature is learned, it becomes less of a temptation to prefer human calculations, easier to base married life on words of the marriage exhortation, ‘The rest is in the hands of God.’”My parent’s role was quite clear and patriotic. “The role of the layman is especially important because we live in a world largely and progressively secularist. It doesn’t deny God or His Church; worse – it ignores them. The Catholic Laity must act to resist the pressures of secularism and worldliness. In America to stand still is to be engulfed”. (104)
As for my father’s second role as Catholic physician, the doctor got a whole 13 page chapter to himself titled “The Doctor in Pre-Cana”. Pre-Cana was the title given to the conferences required of all Catholic couples before being married in the Church. It was at these events that the delicate issue of family planning would be raised.
The instructions in the chapter were quite explicit. The chapter opens with, “The subject of the doctor’s talk in Pre-Cana should be sex, maleness and femaleness, in its broadest and most Christian sense. His approach should be one of respect and reverence toward this mystery – ‘man’s greatest glory in the temporal order’.” There were some cautions as in “There is no necessity of exposing any of the audience to the danger of sinning by an overly-exciting lecture. On the other hand, he must not be apologetic or shy, but after thorough preparation he should speak forth directly and with authority as a Catholic and a doctor.”
Rhetorically again, the Manual asks, “Just what should the doctors attitude towards sex be?” The answer: “The principle that underlies all others is that sex has its primary purpose the procreation and education of the child. Secondarily, it is the most unique expression and symbol of the love of two persons, an intimate act of knowing and giving in which they complete and satisfy each other on every level. This latter purpose, however, is obviously secondary to, and dependent upon, the great reality of the first.”
The Church makes clear its intention to use doctors, in the same manner as pharmaceutical companies, as “learned intermediaries”, with the power to extend and legitimize the Catholic Church “brand”. It reads, “The doctor’s role on the Pre-Cana team is to add his authority, personal and professional, to the teachings of the Church. Speaking with warmth and concern, and yet with a degree of clinical detachment, he can properly take up some areas that priests or layman can avoid. Secondly, his prestige, though often over-rated, can be used to advantage… Finally the doctor can authoritatively counteract many of the popular pseudo-scientific ideas about sex that are gaining currency.”
A few paragraphs later, there is a chilling disclosure reminiscent of the moral dilemma current physicians face with corporate conflicts of interest. It reads, “The doctor has status in our society. He is a combination of scientist and mystic healer. His words carry great weight. You will likely never suspect the tremendous good you will do for Pre-Cana” (read “for pharmaceuticals or medical devices”).
Instructions in the 1957 book on the “Rhythm Method” include considerable verbal gymnastics and “model language and messaging”. First choice, no protection. Second choice, rhythm if you must. Third choice, don’t let a doctor talk you into a “family limitation”.
Fearful facts are provided to defend this approach. “First of all, you don’t know whether you are able to have children at all. Statistics show that about 15% of you will have no children, regardless of what you do, and another 9 or 10% will have at the most one child…It is more difficult to have children than most believe. There are only about 25 to 30 hours in a month when a conception can take place. Therefore, to practice rhythm in the early years of marriage,when you are most fertile, might perhaps deprive you of the blessing of a child.”
And in parenthesis, this special instruction for the doctor: “(The physician must make clear that he is not condemning the use of rhythm by newlyweds on moral grounds, but because it is biologically and psychologically unwise, i.e., it will deprive them of much happiness and success they might achieve in their marriage….If later on the use of rhythm is decided upon it might be recommended that the couple consult their doctor. In passing it might be mentioned that, unfortunately, some doctors are too ready to prescribe family limitations for presumed medical reasons, merely to comply with the desires of the couple.)”
Through the years, my father continued to advance the cause of the “rhythm method” not only to his patients, but also to his daughters and future daughter-in-laws. As a result, my parents eventually had 41 grandchildren, and there would have been more if their children hadn’t finally figured out for themselves what they were doing wrong.
The fact that we were all highly educated, and enjoyed the sense of security of our own personal family safety net thanks to my father’s success as a doctor, tended to accentuate the blessings of our children and soften the occasional bumps and bruises we experienced along the way. Most of our marriages survived. Our families had adequate housing in clean neighborhoods, good nutrition, good schools, reasonable and manageable stress, modest disease burdens, and little hopelessness. Others who my father cared for, whose lives were far less secure, were perhaps not so lucky.
Tags: aca > Cana Conference > Catholic Chrurch > contraception > Obamacare > repealing the ACA > The Basic Cana Manual > Trump care > womens health
Geographic Health Disparity for Abortion Access.
Posted on | October 4, 2017 | Comments Off on Geographic Health Disparity for Abortion Access.

"Code Blue INDEX online"

![]()
![]()
Prospective Health Blog
BIOGRAPHY
NIH Precision Medicine
BIOGRAPHY
Health in 30
BIOGRAPHY
Larry's Letters
BIOGRAPHY
Precision Medicine, Euthanasia, Abortion, Communism, Trillions of Dollars, Losing Freedom, and Town Hall Mobs BIOGRAPHY
Yearning for Universal Coverage Is Not Universal
BIOGRAPHY

