California Dreaming – The World’s 8th Largest Economy Is Not Waiting Around For Trump.
Posted on | April 7, 2017 | 1 Comment

Mike Magee
Health policy experts generally agree that applying taxes to unhealthy products or behaviors can reliably deliver public health benefits. We have learned from the nation’s battle with tobacco that taxes not only discourage consumption but also provide funding for beneficial programs like public health education. In some states and locales, this approach has been embraced as well in the battle against obesity through the use of soda taxes.
California extended healthy taxation within another domain this week – energy. They successfully approved new taxes on gasoline. That action will likely dampen use of carbon creating fuels, accelerate use of high mileage and electric vehicles, and in funding much needed infrastructure for bridge and road repairs decrease injuries related to motor vehicle accidents.
This latest action signals that California, the world’s 8th largest economy at $2.5 trillion Gross State Product, is not waiting around for Congress or Trump’s America to catch up. They have no interest in facilitating his immigration policies or wasting money building walls. Last week, they took the serious step in the early exploration of a single payer health program that would cover all citizens, including documented and undocumented immigrants. And now, they’ve decided to not wait around for the Administration to follow-through on promises of a “huge “ infrastructure bill.
Why should they? Their economy is nearly the size of Brazil (#7 worldwide), and is fueled by record tourism in the south, premier high-tech leadership in the north, and agriculture throughout. Their governor, Jerry Brown, is experienced, progressive, inventive and committed. He’s a grown-up in every way, and has his priorities straight.
Under his care this week, the legislature approved $5.2 billion in gas taxes and vehicle fees by gaining the required 2/3 majority in both the House and Senate state bodies.
In garnering support, the governor focused on the $130 billion in priority repairs and planned new construction on the books that had been accumulating since the last gas tax hike 23 years ago. Brown’s message was simple. direct, and honest: “The Democratic Party is the party of doing things, and tonight we did something to fix the roads of California.”
As we approach the third month of President Trump’s tenure, two things are clear – chaos is not the same as leadership, and the kind of progress we’re seeing in California can fuel growth, optimism and good health. Other states should follow their example.
Tags: California > energy policy > health policy > infrastructure repair > public health programs > taxes
Why Do Canadian Kids With Cystic Fibrosis Live 10 Years Longer Than American Kids?
Posted on | April 4, 2017 | Comments Off on Why Do Canadian Kids With Cystic Fibrosis Live 10 Years Longer Than American Kids?

Mike Magee
At the end of WWII, Canada and the U.S. realized the necessity of focusing on health care infrastructure. There were of course the hundreds of thousands of physical and mental health casualties streaming into overflowing and over-stressed hospitals. Add to this a significant and growing explosion of chronic diseases fed by soldiers and their families embracing tobacco and alcohol, and feeding an explosion of cardiovascular disease, cancers, and psychiatric diseases codified in the first psychiatric classification system, DSM-1.
The Canadians approached the challenge as a planning exercise and ultimately focused on prevention and universal insurance coverage as their starting points. The U.S. took a different road, embracing private scientific enterprise and liberal amounts of national funding to expand scientific research and hospital bed capacity. Insurance coverage in the U.S. was not simply an after-thought. To many, it was a threat, a slippery slope toward socialized medicine, a Communist plot.
Now, more than a half century later, American health continues to suffer. We have been unable and unwilling to “walk back” these decisions, and continue to insist that American scientific brilliance, industrial might, technologic know-how, and massive medical funding will ultimately seize the day. But evidence to the contrary continues to pile up.
Trump’s attempt to dismantle the ACA and downsize Medicaid expansion has boomeranged to the extent that policy analysts have worked hard to expose the negative impacts that would result from eliminating coverage of vulnerable populations. To make their cases, analysts have been exposing some eye-popping comparisons with our neighbors to the north who are all covered under a single payer system.
Case in point: In the March 14, 2017 issue of Annals of Internal Medicine, authors compared the fate of patients followed by the Canadian Cystic Fibrosis Registry to those in the U.S.Cystic Fibrosis Registry. The study included patients from 42 specialty clinics in Canada and 110 clinics in the U.S. Their choice of disease was interesting because it has been a major target of America’s Medical Industrial Complex.
The disease is genetic and incurable, creating excess production of mucous secretions in multiple organs, but especially in the lungs where infected secretions progressively destroy a child and young adult’s breathing capacity. It effects approximately 1 in 10,000 live births in both countries. Effective treatment involves early diagnosis, hands on percussive treatments to clear the mucus, active family and community involvement, break-through pharmaceuticals, and lung transplants for some.
With America’s scientific and technologic might, one would predict that the U.S. would outperform Canada. But here is the sad truth:
1. Canadians with cystic fibrosis live approximately 10 years longer than their counterparts in the U.S. – 50.9 years vs. 40.6 years.
2. The gap in survival has been growing larger over the past two decades.
3. Canadian patients with the disease are afforded lung transplantation with much greater frequency than in the U.S. – 10.3% vs. 6.5%.
4. The factor most directly associated with morbidity and mortality is lack of insurance coverage. U.S. Medicaid patients with the disease fare substantially better than those without insurance.
5. The adjusted risk of death for a patient with the disease in Canada is 34% lower than in the U.S.
6. The newest pharmaceuticals for cystic fibrosis are substantially less expensive in Canada than in the U.S. where some are priced at $250,000 a year.
The Commonwealth Fund authors David Squires and David Blumenthal recently stated that “In medical terms, we might call uninsurance a “comorbidity”—one unique to the United States among all industrialized nations, and just as deadly as pneumonia or diabetes.”
This battle with Trump over the survival of the Affordable Care Act offers a chance to America to start over on health delivery. Scientific know how can not outperform coverage and prevention. That’s been well established. Kids with cystic fibrosis and many other innocents hang in the balance. This is a fight worth having.
Tags: canada health > cystic fibrsis > health care reform > health policy > health reform > U.S. health care
The “Saskatchewan Experiment” – Informing California Health.
Posted on | April 3, 2017 | Comments Off on The “Saskatchewan Experiment” – Informing California Health.

Mike Magee
One of the driving misperceptions about the Canadian health care system is that it is a centrally run and directed delivery system, nationalized from start to finish, top down and authoritarian. That bias, reinforced actively in the U.S., is and has been inaccurate from the start. Understanding this bias could be useful as our nation struggles with the next steps in our own health system evolution.
The Canadian system originated in the province of Saskatchewan, in central Canada. The province had always had a progressive streak and in 1947, in the wake of WW II, launched the first provincial universal hospital insurance plan. The other provinces and territories, as well as the national government, watched the experiment with interest for nearly a decade.
Then in 1957, Canada passed the Hospital Insurance and Diagnostic Services Act which provided 50/50 cost sharing between the federal government and any of 13 provinces and territories that chose to participate in universal coverage of their respective populations.
Seven years later, with all provices and territories voluntarily aboard, Canada’s Royal Commission on Health Services recommended and soon succeeded in launching a comprehensive and universal national health program. Under the system, Canada itself became the sole payer, managing an insurance program universally available to all citizens, including all claims management.
A federal governance body was in charge of standards, but the delivery of care was strictly delegated to the provinces and territories which themselves managed and prioritized annual budgets, and designed their own governance systems.
This commitment to centralized claim management coupled with decentralization and self-determination of budget priorities and delivery of care, now a half century later, continues to define a system which is by no means perfect, but significantly outperforms our own in both quality and cost efficiency.
Our own half century has been tumultuous. But a recent development seems to suggest some desire to start over, and perhaps use the “Saskatchewan Experiment” as a model. I refer to a California bill, SB 562, sponsored by the Califronia Nurses Association. If passed, the state would provide comprehensive medical coverage to all California residents regardless of income or immigration status. There would be no co-pays, no deductibles, no restrictions on provider eligibility.
The plan would not rely on private insurers but would administer claims through a nine-person unpaid board that would be appointed by the California Legislature and the governor. There would also be an appointed health professional and consumer advisory board.
Unlike the small state experience of Vermont (population 620,000), California has nearly 40 million residents, which creates size and scope and diversity to allow for successful risk sharing. As for funding, the state would require a waiver from the federal government to steer Medicare and Medicaid dollars into the state effort. In addition, citizens would pay additional taxes, but they’d no longer have to pay for health insurance themselves.
To many, this sounds like a reach. But a half century ago, so did the “Saskatchewan Experiment”. We should give California a chance. We might like the results.
Tags: California > California SB 562 > Canada health care > health care > health delivery > health reform > Saskatchewan
Who’s The Most Important Doctor-Politician in America?
Posted on | March 31, 2017 | 2 Comments
Dr. Barbara Bollier
Mike Magee
“I’m about health-care’d out.” Those are the words of Sen. Pat Roberts (R.,Kan.)
One can understand his exhaustion. After all, seven years of relentless opposition to the ACA have ended in defeat. The leader, Mitch McConnell, of this effort acknowledged as much last week when he said “It’s pretty obvious we were not able in the House to pass a replacement.” Add to this the ongoing fight in Se. Robert’s own state, where Gov. Sam Brownback has apparently decided that he will be the last man standing when it comes to opposing the ACA in the state of Kansas.
In the federal battle, Republicans have made ample use of two conservative orthopedic surgeons, Tom Price and John Barrasso to attest to the “patient-centeredness” of dismantling a program that has provided or improved the quality of health insurance coverage for 30 million Americans. They have been able to make their appeals with a straight face attesting to their full conversion from physicians to politicians.
No such conversion appears to have seized the hippocratic core of former anaesthesiologist, State Sen. Barbara Bollier (R). Last year, in support of her rural poor uninsured patients of eastern Kansas. After a year of campaigning, she finally gained support for a vote to expand Medicaid under the ACA. She was understandably excited stating, “I am just elated that we’re now at the point that we can debate this bill.”
She was not alone. The Kansas Hospital Association had been a vocal supporter as had the health care organization collaborative, Healthy Kansas, which pegged the job loss title of the Governor’s obstinance at 4000. Polls also indicated that 82% of Kansans supported the ACA Medicaid expansion. State Sen. Laura Kelly cited the 2015 closure of Mercy Hospital in Independence, Kansas as a seminal event labelling the institution “a significant rural hospital.”
A wide range of Kansas legislators agreed. Specifically 81 members of the House and 25 members of the state Senate voted this week for Medicaid expansion. Brownback was unimpressed, vetoing the Bill, saying, ““It fails to serve the truly vulnerable before the able-bodied, lacks work requirements to help able-bodied Kansans escape poverty, and burdens the state budget with unrestrainable entitlement costs.” And with that, 150,000 eligible adults remain uncovered in Kansas.
The Kansas legislature may have had just about enough of their governor. Their roads are falling apart and their credit rating is dropping like a rock, while tax breaks for the rich have hit record highs.
So it’s not surprising that this may be Brownback’s Waterloo. Republican state senator John Doll is in favor of pursuing a 2/3 majority vote to overturn the Governor’s veto. “It’s something we need to do,” he simply says. And they are only 2 votes shy in the Kansas Senate and 3 votes shy in the Kansas House. Signaling their seriousness, the Kansas legislature is in session this weekend.
Tags: aca > Dr. Barbara Bollier > Dr. John Barrasso > Dr. Tom Price > Kansas > medicaid expansion > Sam Brownback
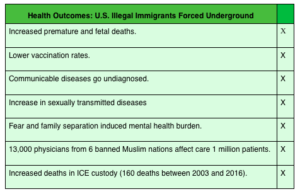
Trump Immigration Impact On Health
Posted on | March 28, 2017 | 1 Comment
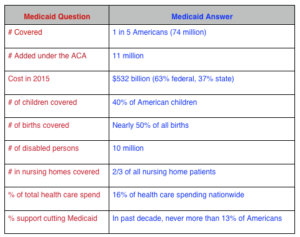
Medicaid: The Base For Single Payer Health Care?
Posted on | March 28, 2017 | Comments Off on Medicaid: The Base For Single Payer Health Care?
“Don’t mess with my Medicaid!” That was clearly the takeaway for Republican legislators heard as they met with hometown crowds in the lead up to their historic Trumpcare defeat. Whether they have “given up the ghost” only time will tell. But as the facts below suggest, going back at Medicaid today means attacking a program with super-majority support.
Tags: aca > Medicaid > Medicaid for all > Obamacare > Republican health care > Ryancare > Trumpcare
Giving Up The Ghost: Republican State Legislators Begin To Acquiesce to Medicaid Expansion.
Posted on | March 27, 2017 | Comments Off on Giving Up The Ghost: Republican State Legislators Begin To Acquiesce to Medicaid Expansion.
Mike Magee
In a recent analysis of the U.S. and Canadian health care systems, two things were clear. First, Canada Health Care was planned, and our’s just happened. And second, both nations favored regional over federal delivery systems. In the U.S., that meant a strong bias toward state management, while in Canada the provinces and territories individually control the majority of funding, coverage, and execution. For Canada this has meant tolerance for variability, which has been counter balanced by a high degree of transparency.
In the U.S., we have preferred more opacity and fudging. Every time we’ve sided with total voluntary participation, we’ve landed with egg on our face. But that has begun to change as last week’s vote on Trumpcare revealed. And Medicaid is where we now see serious cracks in conservative armour.
To review, the ACA when passed in 2010 required that states offer Medicaid to all citizens of the state who fell below 138% of the poverty level ($32,913 for a family of four.) The federal government at first agreed to cover 90% of the expenses for new enrollees and then up’d it to 100%. As we all know, the Republican Congress then loudly announced a call to arms to kill the President’s signature legislation, driving loyal Republicans in state houses everywhere underground. All manners of deception and subterfuge were legitimized for the next 7 years.
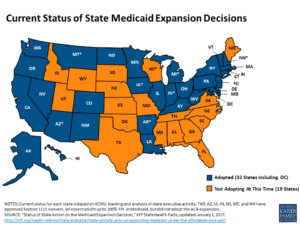
Still, in 31 states and in DC, Medicaid expansion or a federally approved alternative has occurred, including 10 with Republican governors. More importantly, even in the short term (especially with the opioid epidemic surging) the positive health outcomes associated with Medicaid expansion have been dramatic. On multiple measures, the populations covered are healthier, have greater access to care, delay less in getting needed care, visit emergency departments less and are less financially strained. The states budgets have improved as well.
Pragmatic Republican governors like John Kasich delivered direct messages during the Presidential campaign, which might be roughly translated, “Don’t be stupid. Participate and work with the federal government.” The party however chose a different course, which last week ended in disaster.
It now appears that most Republican governors have gotten the message but the Republican state controlled legislatures (many infused with Tea Party loyalists) are seriously lagging behind. A few examples:
Florida: Gov. Rick Scott timidly offered support for a 3 year trial expansion. Florida legislature denied.
Utah: Governor proposed expansion. Legislature denids by adjourning without action.
Wyoming: Governor became a late day advocate. Legislature denied.
Missouri: Governor advocated. Legislature denied.
And then there’s Kansas, whose Gov. Sam Brownback has made some remarkable economic choices that have hurt his state, but he’s still there. He recently became a timid supporter in light of the fact that the state’s own Medicaid funding is “rock bottom” when it comes to coverage. You have to be below 38% of poverty ($9215 for a family of four) in Kansas to qualify for Medicaid. The state’s hospital association just handed the governor an independent study pegging the cost of the state Republican party’s intransigence over the past two years at over $700 million in lost federal funding and an additional 3,400 jobs for the state. Brownback is now “open” to expansion – his Republican led state legislature, not so much.
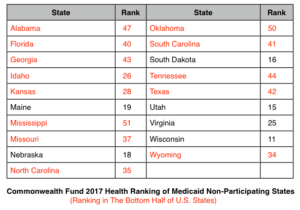
The Commonwealth Fund just came out with their 2017 Health Scorecard which ranks states based on 40 measures of health system performance. Those denying Medicaid expansion showed significantly less progress in measures of access than participating states. As for overall ranks in hold-out states, here they are. 13 of the 19 are in the lower half of states by performance.
In the wake of the Republican failure to repeal the ACA, reports suggest that some state Republican legislatures have gotten the message. North Carolina, Georgia, Idaho, Nebraska and South Dakota are expected to lead the way.
And how about Kansas? Ask Vicki Scmidt, Republican state legislator and chair of their Public Health and Welfare Committee. She said last week before the vote,“If you can predict what’s going to happen in Washington, that would be great if we could be sure what’s going to happen. But in the meantime, we have to move ahead as a state.” Her Democratic colleague added, “I hope the governor gives the people of Kansas what they want.” Seemingly hedging his bets, the governor last week said “I’ll look at whatever they decide to send and whatever the final product looks like.”
Not exactly courageous, but at this point, we’ll mark that as progress.
Tags: aca > health care > health care access > health care reform > health outcomes > Medicaid > Obamacare > trump failures
"Code Blue INDEX online"

![]()
![]()
Prospective Health Blog
BIOGRAPHY
NIH Precision Medicine
BIOGRAPHY
Health in 30
BIOGRAPHY
Larry's Letters
BIOGRAPHY
Precision Medicine, Euthanasia, Abortion, Communism, Trillions of Dollars, Losing Freedom, and Town Hall Mobs BIOGRAPHY
Yearning for Universal Coverage Is Not Universal
BIOGRAPHY

